
Graham Rook er en imponerende vitenskapsmann med lang forsker- og undervisningserfaring. Han var blant de aller første som innså viktigheten av å bringe evolusjonsvitenskap inn i studier av det mikrobielle miljø i relasjon til menneskelig helse og har utviklet en rekke ekstraordinære arbeider på området. I dette intervjuet, gjennomført i 2019 av Eirik Garnås, deler han av sin ekspertise.
1. Please tell us a little about yourself. I’m particularly interested in hearing about your educational background and ‘scientific journey’.

I studied Natural Sciences at Cambridge University, but then decided to qualify in clinical medicine at St. Thomas’ Hospital Medical School in London, so that my research would be orientated towards real human problems. I then started research on the pathogenesis of tuberculosis and leprosy, both caused by pathogenic mycobacteria. During those years neither I nor any other immunologists in that field discovered anything that helped the management of tuberculosis! But we did uncover a lot of interesting biology that led to an interest in Darwinian approaches.
2. How did you first become interested in Darwinian medicine?
We began to realise that most contact with members of the bacterial genus to which Mycobacterium tuberculosis belongs was not harmful, and might even be beneficial. For example, Danish workers found that the BCG vaccine provides health benefits and increases overall survival by mechanisms that have nothing to do with protection from tuberculosis. Other workers suggested that even M. tuberculosis itself might have helped evolving humans to survive, because it synthesizes nicotinamide and so might prevent pellagra in starving protein-deficient hunter-gatherers.
Meanwhile we found that human immune systems learn to recognise the hundreds of saprophytic mycobacterial species present in the local environment, and in collaboration with Chris Lowry (now in Boulder CO) we discovered that immunising mice with a harmless environmental saprophyte named Mycobacterium vaccae influenced serotonergic neurons in the brain.
More recent collaborations on this have shown that these mice become resistant to detrimental effects of a severe psychosocial stressor. Vaccination with M. vaccae blocks the distortion of the gut microbiota, the colitis and the behavioural changes that occur in unvaccinated control animals exposed to the stressor. All of these effects of M. vaccae depend on induction of regulatory T lymphocytes (Treg). These experiments alerted us to the fact that exposure to environmental microorganisms is important for the correct functioning of the mechanisms that regulate the immune system.
3. By now, it’s well-established that the human immune system depends on inputs from bacteria, fungi, helminths, and other small life forms in order to function appropriately. What made you initially realise that this is the case, and how did you go about mapping the nature and evolution of this relationship between man and microbes?
While we were studying the effects of exposure to harmless environmental organisms, the medical profession was becoming increasingly aware of the fact that two classes of illness were increasing dramatically in Western, particularly urban, communities.
First, there are what I call the “forbidden target” diseases where the immune system is attacking things it should not attack: i) our own tissues (autoimmune diseases), ii) trivial harmless allergens (allergic disorders) or iii) the gut contents (inflammatory bowel diseases).
Secondly there are the “persistent inflammation” diseases where biomarkers of inflammation (CRP, IL-6 etc.) remain raised despite the absence of any infection or other valid reason for immune activity. Persistent inflammation is associated with i) metabolic, ii) cardiovascular, and iii) psychiatric disorders. (The latter point links to the M. vaccae work outlined above).
All of these disorders suggest a problem with regulation of the immune system. Since all known immune attack mechanisms are involved in one or other of this list of disorders, the problem was clearly one of broad immunoregulatory activity, and not merely an imbalance between Th1, Th2 or Thwhatever effector pathways as had originally been proposed. We also knew that the failure of immunoregulation could not be due to reduced exposure to common childhood infections in modern urban societies because these (measles for example) are “Crowd Infections” that did not affect human populations until very recently, and could not evolve a relationship with humans that made them a necessity. Measles kills you or makes you solidly immune, so it could not persist in evolving hunter-gatherer groups.
We therefore asked ourselves which microorganisms would have inevitably been encountered by evolving humans. Often things that are inevitable for long evolutionary periods become incorporated into our physiology as necessities. We already had evidence that some environmental organisms (mycobacteria) were helpful and we soon realized, thanks to superb work by many laboratories, that the symbiotic microbiota was also crucial.
Finally, under some circumstances (see comment after question 6 below) certain “Old Infections” such as tuberculosis, Helicobacter pylori or helminths might also be useful. (Unlike the Crowd Infections, the “Old Infections” were able to persist for life in isolated hunter-gatherer groups without killing the host). So the “Old Friends Hypothesis” was born, suggesting that exposure to maternal microbiota, organisms from the natural environment, and some Old Infections, might be essential for the correct development of the immune system.
4. Evolution via natural selection brings about organismal adaptation to environmental settings, including its biotic components (e.g., microbial life). One of the principle tenets of Darwinian medicine is that biological evolution often (but not always) is a slow process and that when environmental conditions change, organisms may suffer as a result of being poorly suited to the new conditions. This is very relevant in the context of human health and well-being, as our environment has changed dramatically recently, particularly in the time that has passed since the Agricultural Revolution, and even more so the Industrial one. Part of this change involves altered exposure to microbes and worms. Could you briefly summarize the nature and implications of this transition of the man-microbe relationship?
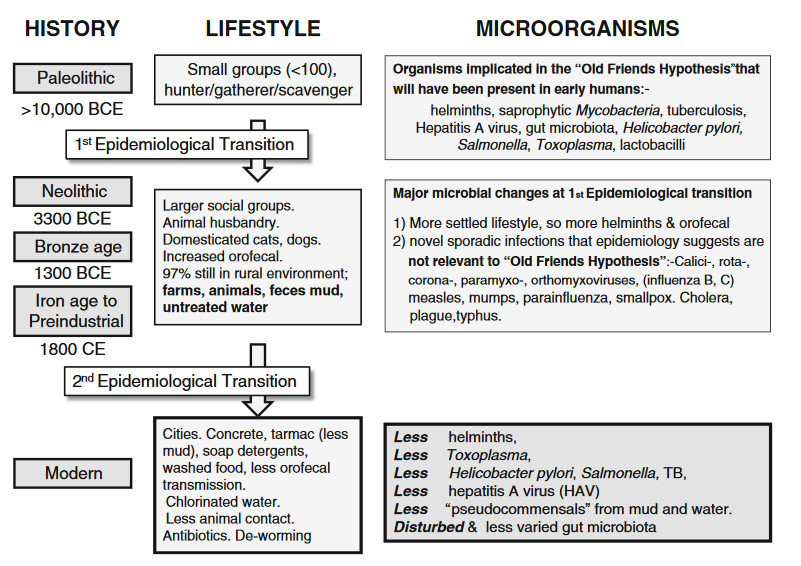
For several years there was a tendency to believe that the critical factor reducing our microbial exposures was hygiene. This led to some terrible nonsense that has probably killed some children. When we think in terms of the Old Friends the situation become clearer. We can now list many factors that alter our exposures to the relevant microorganisms, and hygiene does not appear in the list except to the extent that some inappropriate hygiene practices limit transmission of maternal microbiota to the infant.
- Antibiotics during pregnancy.
- Antibiotics during early life
- Caesarean delivery
- Lack of breast-feeding
- Inappropriate hygiene that limits transmission of microbiota to the infant in early life
- Unvaried diet.
- Diet lacking fibre (plant cell walls).
- Lack of exposure to the natural environment
- Supermarket food depleted of environmental microorganisms
- Distortion of the environmental microbiota
- Pollutants
- Urbanisation
- Industrial and agricultural chemicals (Note that glyphosate was first patented as an anti-bacterial)
These factors are additive, and working together they severely disrupt the microbiota and the crucial “educational” inputs to the immune system, the need for which is explained below.
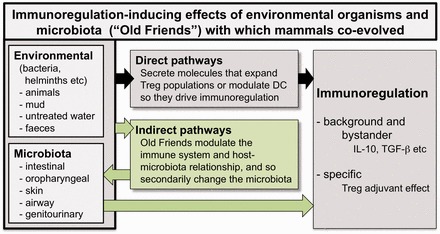
5. It’s not surprising that we’ve come to tolerate life forms that were routinely present in the natural environments in which we evolved. What’s more interesting is how and why such ‘old friends’ have come to be so critical with respects to the workings of the human immune system. Could you briefly talk a little about that? I’m particularly interested in hearing you explain, from a Darwinian point of view, why mammals such as ourselves have come to rely on other organisms for proper immunoregulation. Is the key point simply that it’s “cheaper” and requires less energy to utilize something that’s already there (e.g., substances produced by bacteria) than it is to evolve sufficient capabilities to do everything oneself, or are other explanations more compelling, as you see it?
Vertebrates evolved an extremely complex gut microbiota that is in intimate contact with the gut wall. These organisms (about 1014 of them) contain DNA that collectively encodes at least 100x more enzymes and metabolic pathways than are encoded in our own genomes. Since the microbiota can evolve and change rapidly, whereas human evolution is slow, the microbial genomes give us rapid flexibility and adaptability. Moreover, as we co-evolved with these microbial communities, many microbial products were co-opted to play roles as signals for the development and function of essentially all organ systems, including the brain.
However, the existence of this complex microbiota gave the vertebrate immune system a problem. How was it to “farm” and control the vast number of species in the microbiota while simultaneously fighting off pathogens that attempt to invade our tissues or to upset the human-microbiota symbiosis?
It was not possible to build a sufficient repertoire of receptors to recognise a vast and rapidly changing array of microbial molecules by simply duplicating receptor genes and evolving variants. This would have added enormously to the size of the genome, and in any case, it was too slow. Such a mechanism could never keep up with microbial evolution. Therefore the “adaptive” immune response appeared. (Invertebrates, with their simpler microbiotas, do not have this type of “adaptive” immune system).
The adaptive immune system generates a vast repertoire of receptors (antibodies for example) by mutation, so few genes are required. Thus a new repertoire is generated de novo in each individual. Then lymphocytes bearing relevant receptors are selected and clonally expanded, while useless ones, or any that recognise the individual’s own tissues, are eliminated.
How are relevant receptors selected? This is too complex to explain in full here, but part of the mechanism depends on exposure to as many microorganisms as possible. Thus the adaptive immune system develops a repertoire that is relevant to the microbial environment in which the individual lives, rather than to a microbial environment from the distant past, but to develop this repertoire it must have an “educational” input of microorganisms from the gut and the environment.
But this not the only reason that the immune system needs microbial exposures. I list some more below:
- Exposure to microorganisms that can colonise the microbiota.
- Exposure to spores of human gut-adapted strains, deposited in the environment by past generations.
- Horizontal gene transfer: gut microbiota readily pick up DNA from other organisms. This can supply required enzymes to cope with dietary change
- Microbial molecules, such as LPS, that provide signals to the developing immune system.
Item 5 requires further explanation. It seems that the airways and gut require exposure to microbial inflammation-inducing components to set up the right level of background inflammation, and the right level of anti-inflammatory mechanisms (such as a molecule known as A20). Perhaps this acts as another “testing” of the environment into which the individual has been born, so that background activity and immunoregulation are matched to that environment, and appropriately balanced.
6. Most people are probably open to the idea of bringing new microbes into their lives; however, many are probably resistant to inoculating themselves with worms. Why are non-microbial ‘old friends’, such as certain types of helminths, important in the context of human immunoregulation? What do they do that microbes can’t or don’t?
I now suspect that we do not need worms! I have changed my opinion on this as explained in my recent Lancet article. Helminth infections are enormously varied. Some exist in the tissues, others in the gut, or in the blood. Moreover, the species with which people were infected was also very variable, and even in villages situated quite close together, the helminth load can be quite different. Moreover, and most important of all, different helminths evolved a multitude of different mechanisms to suppress our immune responses.
Therefore it is remarkably unlikely that the immune system could evolve dependence on something so varied and inconstant. To what exactly would it adapt? I now believe that if a mother is infected with helminths, and passes these on to her child, that child will have some epigenetically encoded dependence on the presence of the helminth, which will have usurped some immunoregulatory functions. So deworming such an infant might promote, for instance, the risk of allergies. But in rich Western urban environments, after a few generations, this epigenetically encoded dependence will disappear. I suspect this is why clinical trials using helminths are giving disappointing results…..but more trial results are due.
7. Early life is a critical window with respects to maturation and development of the immune system. As you see it, to what extent is it possible for grown-ups to remedy issues that may have emerged partly or largely as a result of improper exposure to bacteria, parasites, etc. early in life?
This is a difficult question. It is absolutely clear that there is a window of opportunity in the first weeks or months of life during which an appropriate gut microbiota needs to be in place. We know that this is necessary for maturation of the immune system and the metabolic system in animals and humans. Things that disturb the microbiota during this critical period (antibiotics for example) increase the risk of obesity and allergic disorders, and probably of other inflammation-related disorders. too.
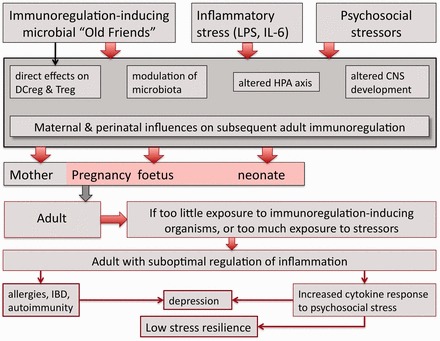
Germ-free mice also have abnormal brain function and abnormal stress responses that cannot be corrected by reconstituting the microbiota in adulthood. We don’t know if the brain is affected similarly in humans, though as stated earlier, we do know that persistent systemic biomarkers of inflammation are associated with psychiatric disorders.
In adulthood the disturbance to the microbiota seems to correct itself, but we cannot be sure that the physiological systems that mature early in life can ever recover. As mentioned, above, the development of the brain and stress responses in germ-free mice does not recover in adulthood if the microbiota was deficient during the critical early window of opportunity.
We need more epidemiology to answer these questions in relation to humans. Moreover, although the microbiota seems to recover according to the data we have now, the fact is that we are only looking at a fraction of all the organisms there. We cannot be sure that organisms that are crucial, but present in small numbers are restored later in life.
8. As you see it, how should we go about rebuilding the ecosystem of the human body and making human-microbe relationships more harmonious? Are there any strategies or therapeutic solutions that you feel particularly strongly about, either ones that are already available to the public, or that one day may become available? Any recommendations for severely immunocompromised individuals and/or just the average Joe who wants to augment his immune system?
At the current state of knowledge all we can say is that we should do what we can to avoid the causes of diminished microbial exposure listed under question 4. So we should aim for:
- Natural deliveries and breast feeding, with minimal antibiotic exposures.
- A varied, fibre-rich diet.
- Legislation to minimize exposures to industrial and agricultural pollutants that alter the microbiota of the environment, animals, plants and food.
- Plenty of exposure to the natural environment (run round a park rather than exercising in an urban gym).
- Increase green spaces in cities, particularly spaces providing access for less wealthy sections of society. These can be quite small, around bus stops, or on rooftops or walls.
- Education of the public and the media.
Meanwhile we also need much more research and “big data” approaches to understanding the roles of the microbiota in greater detail. This probably requires documenting the metabolome of the entire microbiota, which might prove more directly relevant than a list of microbial strains. We still know only a small percentage of all the organisms present, so there could still be crucial disease-causing or disease-preventing strains that are not yet known.
We still don’t know how many illnesses might be treatable by modifications of the microbiota, or microbiota transplants.
9. Have you made any new and intriguing discoveries recently, or come to an exciting realization? If so, it would be great if you could tell us a bit about it.
A whole series of deliberate genetic modifications of mice that alter the immune system have been shown to cause inflammatory disorders. No surprise there. But what is astonishing is the fact that these inflammatory disorders can often be transferred to normal mice, that have not undergone the genetic modification, by simply reconstituting the microbiota of the normal mice with the microbiota of the genetically modified sick animals. If this principle is true for humans too, then the persistence of many illnesses might turn out to be due to secondary changes to the microbiota rather than to the original cause of the illness.
Our work with M. vaccae and mice subjected to a stressor has emphasised this point. So now I am fascinated by the increasing evidence that behaviour mimicking depression, and even schizophrenia, can be transferred from human patients to germ-free or antibiotic-treated normal rodents. Is a treatment revolution in sight? Only more research can answer this.
10. What do you consider to be the most important things Darwinian medicine has to contribute to the health care system?
I would rather keep within my own field! The Darwinian approach has taught us that we are ecosystems containing humans and numerous categories of microbes with which the human component of the ecosystem has co-evolved. We are not individuals. Looking at the problem in a Darwinian way immediately points to the organisms that we must have evolved to encounter, and enables us to understand why these organisms have the functions in our physiology that we observe. The potential for disease prevention or treatment is vast, but still unexplored.
Mer fra Graham Rook…
Utvalgte bøker
- The Oxford Handbook of Evolutionary Medicine (inneholder kapittel om immunforsvaret skrevet av Rook)
- The Hygiene Hypothesis and Darwinian Medicine
Utvalgte vitenskapelige arbeider
- «The Microbiota, Immunoregulation, and Mental Health: Implications for Public Health«
- «Time to abandon the hygiene hypothesis: new perspectives on allergic disease, the human microbiome, infectious disease prevention and the role of targeted hygiene«
- «Hygiene and other early childhood influences on the subsequent function of the immune system«
- «Microbial ‘Old Friends’, immunoregulation and stress resilience«
- «A Darwinian View of the Hygiene or“Old Friends” Hypothesis«
- «99th Dahlem Conference on Infection, Inflammation and Chronic Inflammatory Disorders: Darwinian medicine and the ‘hygiene’ or ‘old friends’ hypothesis«
